Neurosurgeon vs Cardiothoracic Surgeon Career Battle: Which Path Is Best for You?
Most careers in medicine are demanding. Neurosurgery and cardiothoracic surgery take that to a completely different level. Learn which path is best for you.
For decades, Step 1 was the single most dreaded exam in all of medical education.
You thought the MCAT was brutal? Step 1 made it look like a warm-up.
For many students, preparation started nearly a year in advance. Months of steady build-up eventually culminated in 2 to 3 months of intense, full-time studying. Twelve-hour days. Six days a week.
Your future compressed into a three-digit number.
The toll was enormous. Students’ mental health deteriorated. Burnout was rampant. And the calls for change grew louder.
Then, in 2020, the announcement came: Step 1 would go pass/fail.
The announcement sparked an immediate and heated debate. Online medical forums erupted. Students, residents, and physicians argued that making Step 1 pass/fail would finally address burnout, improve mental health, and fix a broken system. Deans and institutions echoed similar hopes. Students exhaled for the first time in years.
Except there were voices saying: you’re confusing the symptom with the cause.
Step 1 wasn’t the disease. It was a thermometer measuring a much deeper problem. And removing the thermometer doesn’t cure the fever.
Three years later, the data is in. And it tells a very different story than the one everyone expected.
So, was turning Step 1 pass/fail a mistake?
To understand how this went wrong, you need to understand what Step 1 actually did.
Before it went pass/fail in 2022, Step 1 was a single, high-stakes exam taken between second and third year. It tested foundational medical knowledge, but more importantly, it functioned as a sorting tool.
A higher Step 1 score shaped which specialties you could realistically pursue, which programs would consider your application, and how early you could gauge your own competitiveness. For better or worse, you knew where you stood.
Residency programs face overwhelming application volume. They need fast, standardized filters just to function. Step 1 filled that role for decades.
When critics argued that too much weight was being placed on a single test, the logic behind pass/fail seemed straightforward. Remove numeric scores and reduce pressure.
But removing a primary filter doesn’t eliminate pressure. It redistributes it.
The intention behind pass/fail was to reduce stress. But the debate missed a bigger question: what happens to the rest of the system when you remove one of its primary filters?
Making Step 1 pass/fail didn’t change the stakes or how competitive programs are. It removed an early objective benchmark.
Mess up Step 1 in the past? You could make real improvement on Step 2 CK. Mess up Step 2 CK now? That’s your only shot.
So what actually happened?
Pass rates dropped by about 5 to 7 percentage points, with a larger decline among DO students.
Before pass/fail, US MD students had pass rates around 95-97%. By 2023 and 2024, that dropped to roughly 89-91%.
That means about 1 in 10 MD students now fail Step 1, compared to roughly 1 in 20 before.
For DO students, the decline was steeper. Pass rates fell from the low 90s into the mid-to-high 80s, a drop of about 6 to 8 percentage points.
What changed?
Lower stakes change behavior.
When an exam feels less impactful, preparation becomes more variable. Some students still over-prepare. Others pull back. That variability increases the risk of failure at the margins.
Removing the incentive to excel also removed the buffer against failing.
And there’s another factor most students don’t consider. On the exact same day Step 1 went pass/fail, the USMLE raised the minimum passing score from 194 to 196. Students were preparing less intensely for an exam that had actually become harder to pass. Less preparation, higher bar, same day. The result was predictable.
But the stress didn’t disappear.
Recent studies of students approaching Step 1 in the pass/fail era still show high levels of anxiety and poor sleep. Even without a numeric score, Step 1 remains a major psychological stressor.
The experience didn’t become calm or low-pressure. It just changed shape.
There were two major pressure shifts. The first is the most obvious.
Step 2 CK has become the primary numeric test score differentiator in residency selection.
Scores didn’t suddenly rise faster after 2022. They were already trending upward. What changed is how heavily programs depended on them.
The timing of Step 2 didn’t change either. Step 2 CK is still taken after third-year clinical rotations, usually with a short dedicated study period. But that means much of your studying overlaps with long work hours, evaluations, and residency applications. That concentrates more pressure into a single exam during one of the busiest periods of medical school.
When Step 1 became pass/fail, many students reallocated their time. Some pulled back on Step 1 prep and spent more time on research and extracurriculars. For some students, that shift meant less consistent Step 1 preparation, increasing the risk of failing.
Residency programs didn’t stop needing filters. They still have to sift through thousands of applications. Removing one numeric metric didn’t eliminate the need for sorting. It meant programs leaned more heavily on the remaining ones.
Now there’s more pressure on a single exam with no “backup test” to offset a weak Step 2 performance. This translates into fewer opportunities to recover and more downstream consequences from a single bad outcome.
Knowing what matters isn’t the same as knowing how to prepare for it. Most students hit a plateau, stuck around a 245, grinding through more and more practice questions and content review, hoping their score will eventually climb. It won’t. Not without changing the approach.
When Step 1 was still numerically scored, most students didn’t spend months studying for Step 2 CK. Dedicated periods were often only a few weeks long. I studied for three and a half weeks and scored 269. Students today are spending multiple months and not hitting that number. The difference isn’t intelligence or effort. It comes down to three pillars that most people don’t fully understand: content knowledge, study strategies, and test-taking skills.
On the Med School Insiders Blueprint channel, we dig into the strategies that actually move the needle based on our experience helping over 10,000 students succeed.
Almost everyone over-indexes on content knowledge, sticking to more questions, more review, more memorization. That’s something you can largely do on your own time, and yes, we can help clarify things when students are confused on tougher topics, but that alone isn’t what moves the needle quickly.
What actually causes the biggest score improvements are the other two pillars. Better study strategies feed directly into stronger content knowledge, so you’re learning more efficiently without grinding harder. In other words, learning faster and forgetting slower. But the real lowest-hanging fruit?
Test-taking skills. This is where students leave the most points on the table, and it’s the area almost no one optimizes properly.
It’s knowing how to approach a question when the answer isn’t immediately obvious. How to eliminate choices strategically. How to make better guesses when you’re unsure. How to read questions with intent instead of reacting to surface details. And how to manage pacing so you never run out of time.
If you want help identifying which of those three pillars is holding you back and how to increase your score in the quickest way possible, book a free strategy call, and we’ll talk about whether or not you’re a good fit for our program.
So what was the next major pressure shift?
Research didn’t suddenly matter after Step 1 went pass/fail. It was already increasing. But the slope changed dramatically.
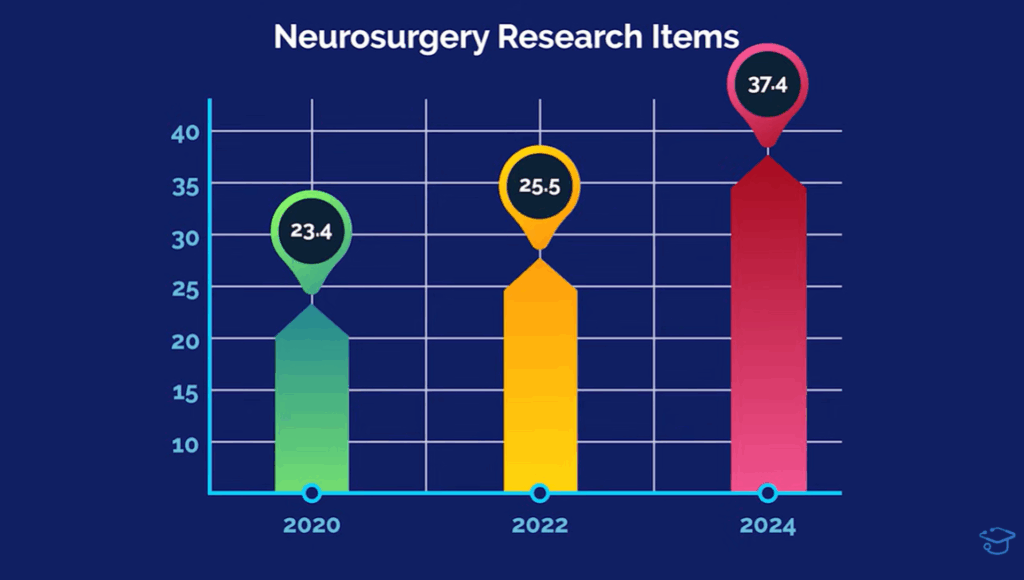
According to NRMP Charting Outcomes data, in neurosurgery, matched applicants averaged 18.3 research items in 2018. In 2020 it was 23.4. By 2022, that climbed to 25.5. But from 2022 to 2024, it jumped to 37.4. That’s nearly a 12-item increase in half the time.
Plastic surgery more than doubled, from 14.2 to 34.7. Orthopedics went from 11.5 to 23.8. Dermatology reached 27.5.
This isn’t gradual inflation. This is an arms race.
When Step 1 scores were removed, residency programs didn’t suddenly become holistic. They still needed ways to filter thousands of applications. With fewer early objective signals, research output became one of the remaining measurable differentiators.
As a result, incentives shifted. Research became more heavily weighted, and the system began rewarding the countable output of research items, including abstracts, presentations, and publications, over depth alone.
Beginning with the 2027 cycle, ERAS will replace the traditional Publications section with a new Scholarly Work section. It introduces clearer categories, allows applicants to designate select items as most meaningful, and is designed to shift emphasis from sheer volume to substance and depth of contribution.
But structural incentives haven’t changed. Programs must filter. Research metrics, authorship position, publication type, and journal relevance remain fast proxies for academic engagement and productivity.
The format may change. The filtering pressure does not.
The original promise was reduced stress.
But burnout and anxiety persist because burnout was never primarily about Step 1.
What actually changed was how students are evaluated, not how competitive residency remains. There’s less early clarity. Fewer objective benchmarks. Less time to adjust once signals appear.
Competitive things are competitive.
Changing something to pass/fail doesn’t make the end goal less competitive. It changes the metrics by which you play the game.
Residency didn’t become less competitive when Step 1 went pass/fail. The competition shifted to different signals, ones that show up later, carry higher stakes, and are harder to recover from.
The most competitive specialties consistently cluster at the top. Dermatology, plastic surgery, orthopedic surgery, neurosurgery, and ENT stand clearly above the rest in terms of applicant pressure, score expectations, and research volume.
Other specialties like radiology, radiation oncology, and anesthesiology are competitive, but not in the same tier as those top five when you look at objective match data.
Meanwhile, specialties like family medicine and pediatrics generally face less intense screening pressure because their supply-demand dynamics differ fundamentally.
This distinction matters because competition in medicine isn’t abstract. It’s driven by incentives. Where demand far exceeds supply, programs will always rely on hard filters, regardless of whether Step 1 is scored or pass/fail.
Programs must filter. Application volume makes detailed review impossible. When one signal is removed, others take its place.
A lackluster Step 2 CK score is now much harder to recover from. Research output carries far more weight. And programs lean more heavily on clerkship grades, letters of recommendation, and institutional familiarity to sort applicants at scale.
Take Step 1 seriously, even though it’s pass/fail. It’s about finding the right balance.
Investing too much energy into Step 1 puts you at a disadvantage because while you’re hyper-focused there, other students are building research, publications, and competitive signals. Aim to be comfortably above the danger zone, but don’t overprep at the expense of the rest of your application.
Treat Step 2 CK as the primary exam in residency screening.
Start research early and be intentional. Focus on meaningful contributions, not just checking boxes.
Understand how the specialties you’re considering actually evaluate applicants, including what Step 2 scores are typically expected.
Step 1 going pass/fail didn’t reduce competitiveness. It redistributed it.
If you’re wondering where you actually stand for the specialties you’re considering, plug in your stats at SpecialtyPredictor.com to see your odds of matching based on the latest official NRMP data.

Most careers in medicine are demanding. Neurosurgery and cardiothoracic surgery take that to a completely different level. Learn which path is best for you.
The 2027 ERAS cycle runs from June to the following May. Here’s exactly what to work on each month, from Step 2 CK through Match Week.