Signs You’re Wired to Become a Psychiatrist
We’re breaking down the six signs you’re wired for psychiatry, and the one thing that will tell you faster than any rotation whether this career is for you.

Dr. Patel’s shift ended three hours ago. But she’s still at the hospital—charting, returning calls, doing the work of three people.
One colleague just quit. Another’s out on stress leave. And there’s no replacement in sight.
This wasn’t what she signed up for. She wanted to care for people, not be worn down by the tedious minutiae of a bureaucracy in shambles.
And it’s not just her. This is happening in hospitals across the country.
Because the truth is, we’re running out of doctors.
And it’s about to get worse.
We’re staring down the barrel of a massive physician shortage in the US—an estimated gap of 187,130 doctors by 2037. That’s not just a staffing issue. That’s a public health crisis in slow motion.
So what’s driving this shortage? And what does it mean for the future of medicine?
The doctor shortage isn’t just a prediction. It’s already here. In 2017, experts were warning about the impending shortage of doctors—over 100,000 physicians by 2030, which is right around the corner.

But what’s even more alarming is the latest projection: by 2037, that shortage could nearly double. And this deficit is spread across almost every specialty in medicine.
Now, a quick caveat here: counterpoints suggest agencies like the AAMC might be incentivized to inflate these numbers, and other organizations may have more conservative estimates. But even if you take a more conservative view, the projected shortage is still an undeniable crisis.
Primary care is going to take the hardest hit. By 2037, we could be short 87,000 primary care doctors. But it doesn’t stop there. Critical specialties, such as OB/GYN, cardiology, and anesthesiology, are also facing shortages.
What does this mean for patients? Longer wait times, delayed diagnoses, and more people being forced to go without care, especially in rural areas. Entire communities could become medical deserts, where access to even basic healthcare is a luxury.
By 2037, rural areas will be short 60% of the physicians they need, compared to just 10% in cities. And it’s already happening. Right now, as we speak, 76 million Americans are currently living in primary care deserts, and most of them are in rural communities.
So, how did we end up in this mess?
Unfortunately, it’s not just one factor. Let’s break it down.
Let’s start with demographics. The US is aging rapidly.
By 2030, every single Baby Boomer will be 65 or older.
As people age, they require more healthcare, typically for more complex and long-term conditions. The number of people aged 75 and older is expected to grow by 55% by 2036.

And it’s not just the patients getting older—it’s the doctors too.
Nearly half of all practicing physicians in the US are already over 50 years old, and one in five are over 65.
That means a huge wave of retirements is right around the corner, shrinking the number of available doctors just as demand is exploding.
Next up: medical training.
Back in the ’80s, we were actually worried about a doctor surplus.
That led to the 1997 Balanced Budget Act, which capped the number of residency slots funded by Medicare. And those caps are still in place today, creating a huge bottleneck in the pipeline of new doctors.
Every year, hundreds of qualified medical school graduates get stuck in limbo because they can’t secure a residency spot to complete their training.
After being handed a medical degree, they’re told, “Sorry, you can’t work yet.”
Additionally, specialized residency programs and fellowships are heavily concentrated in major cities, yet 18% of Americans reside in rural areas, where only 2% of Medicare-funded residency slots are available.
This further hinders underserved areas where the need is greatest.
The next contributing factor is the cost of becoming a doctor.
The average medical student graduates with over $260,000 in debt—a significant financial burden, even with a high-earning career ahead.
And while many physicians can manage and pay off this debt over time, especially with smart financial planning, keep in mind that $260,000 is only the average. Many graduates face upwards of $400,000 in debt, particularly if they attended private institutions.
For someone considering medicine, that kind of debt can feel daunting, to say the least, especially if you’re from a lower-income background or want to go into primary care, which pays less than other specialties.
If that wasn’t enough, there’s more trouble ahead.
Proposed changes to federal student loan programs could dramatically exacerbate the situation.
The 2025 budget proposes capping Direct Unsubsidized Loans at just $150,000, which is nowhere near enough to cover the full cost of medical school for many students.
They’re also considering eliminating key loan forgiveness programs, such as Public Service Loan Forgiveness, or PSLF, for residents.
That’s a huge blow, particularly for those who planned on working in underserved areas.
Even the proposal of these changes is a slap in the face to anyone hoping to pursue medicine.
Now, what happens if this shortage continues unchecked?
We don’t even have to speculate—we’re already seeing the impact.
Longer wait times, missed diagnoses, and far too many people being forced to go without even basic care.
And once again, it’s rural areas that are being hit the hardest. Entire labor and delivery units are shutting down, forcing women to travel massive distances to give birth.
And let’s not forget the mental health crisis. Behavioral health services are already in short supply, and with fewer doctors, it’s only going to get worse.
The downstream effects are deadly, too. Coming as no surprise, studies show that areas with fewer doctors have lower life expectancy and higher rates of chronic illness.
Which brings me to another uncomfortable truth: the US spends far more per capita on healthcare than any other high-income country. Last year alone, healthcare spending in the US hit a whopping 5 trillion, or nearly $15,000 per person. And what do we get for that? Ranking dead last on many key health indicators.
In fact, our average life expectancy is more than four years below the 10-country average, behind countries like Canada, France, and Germany. We’re spending the most, and yet we’re dying sooner and living less healthy lives. That’s the brutal reality of our system.
Are doctors to blame for astronomically high healthcare costs? We broke down the truth about healthcare spending in a previous guide.
And the doctors still in the system are overwhelmed.
Workloads are increasing, hours are longer, and burnout rates are rising.
This creates a vicious cycle: the more stress doctors face, the more likely they are to leave the field, and the harder it becomes to attract new talent.
And tragically, the stress is taking a heavy toll.
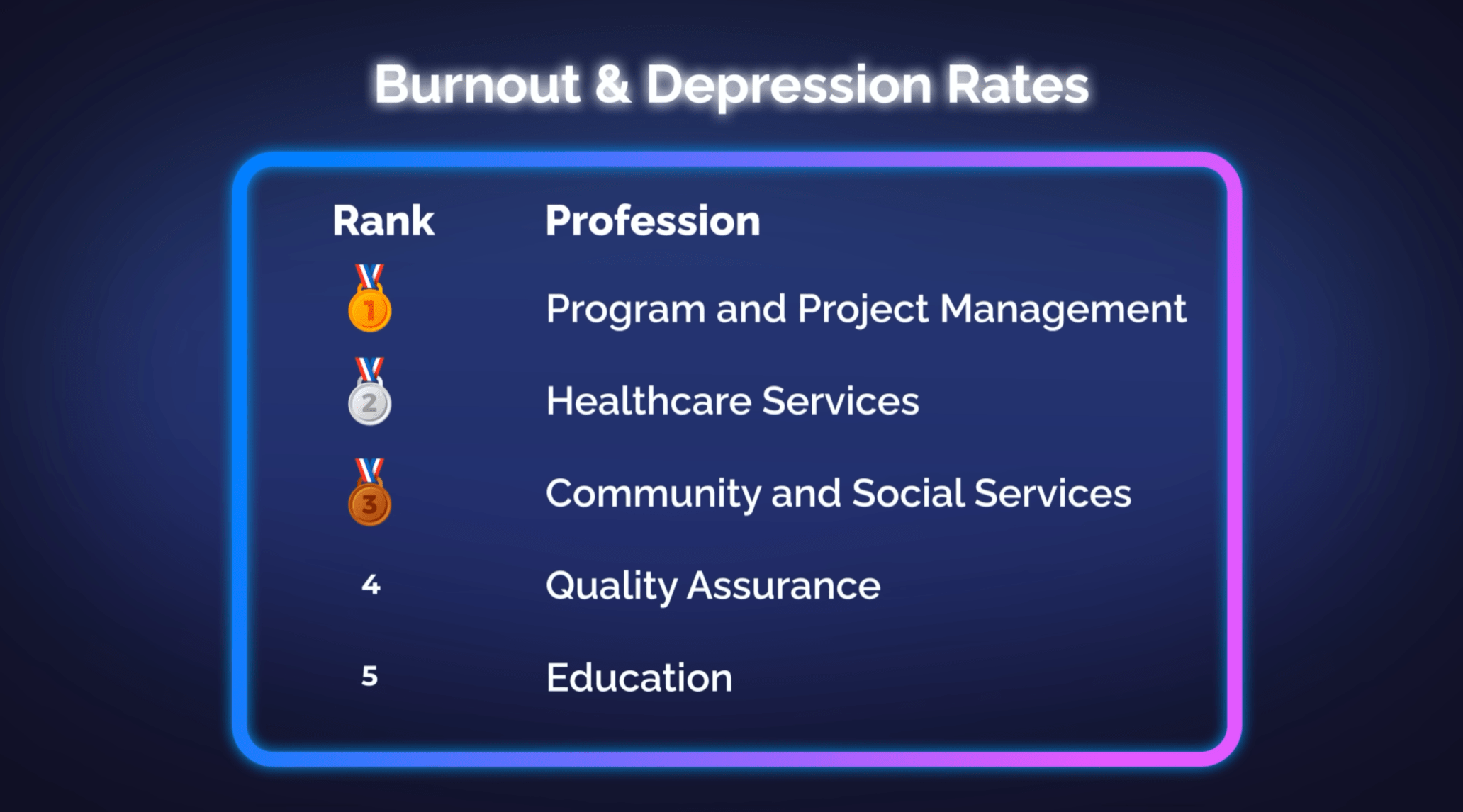
Physicians have one of the highest rates of burnout and depression among any profession, with 300-400 doctors taking their own lives each year.
Now that we understand the mess we’re in, what can we do to fix it?
One of the most critical areas for reform is graduate medical education, or GME.
We need to expand residencies—big time. That means lifting the cap on Medicare-funded slots and investing in training programs in rural and underserved areas.
Congress has added 1,200 new GME slots since 2021—the first increase in decades—but that barely scratches the surface. We need thousands more.
But broader efforts on residency reform haven’t made much progress.
Take, for example, the 2014 Institute of Medicine report.
It recommended shifting residency funding toward value-based care rather than the traditional fee-for-service model. But like many healthcare reforms, it was ultimately blocked by political resistance and powerful interest groups.
We break down the difference between value-based and fee-for-service care in a previous video—link in the description.
We also need to make med school affordable again.
That means protecting loan forgiveness programs like PSLF, expanding service-based scholarships, and increasing support for students from socioeconomically disadvantaged backgrounds.
We also need to rethink how we compensate doctors. This is especially true in primary care, where salaries often don’t reflect the vital role these physicians play.
But doctors need more than money—they need respect, autonomy, and support.
That means:
But what about a more immediate solution to bump up our physician numbers?
One of the fastest and most readily available answers might be right in front of us: international medical graduates, or IMGs.
Streamlining the licensing process for IMGs could help address critical shortages, particularly in underserved areas.
IMGs already make up about 25% of the US physician workforce and can help fill immediate gaps.
And finally, AI and telemedicine can help. But only if we use them wisely.
AI can cut down on charting and help flag health risks early, and telemedicine can bring care to rural communities.
The real question now is: Will action be taken before the system collapses, or only after it’s too late?
The future of medicine is more unpredictable than ever before. To stay ahead of the curve and up to date on critical topics that affect your career, health, and happiness in medicine and beyond, subscribe to our weekly newsletter.

We’re breaking down the six signs you’re wired for psychiatry, and the one thing that will tell you faster than any rotation whether this career is for you.

We recommend applying to 25-30 medical schools. Here’s how to split that list across reach, target, and safety schools, plus the real costs to expect.