
12 Niche Doctor Specialties You Didn’t Know Existed
Medicine is a much wider field than most people realize. These are 12 niche doctor specialties you’ve probably never heard of.

There’s a lot more to anesthesia than putting people to sleep and waking them up.
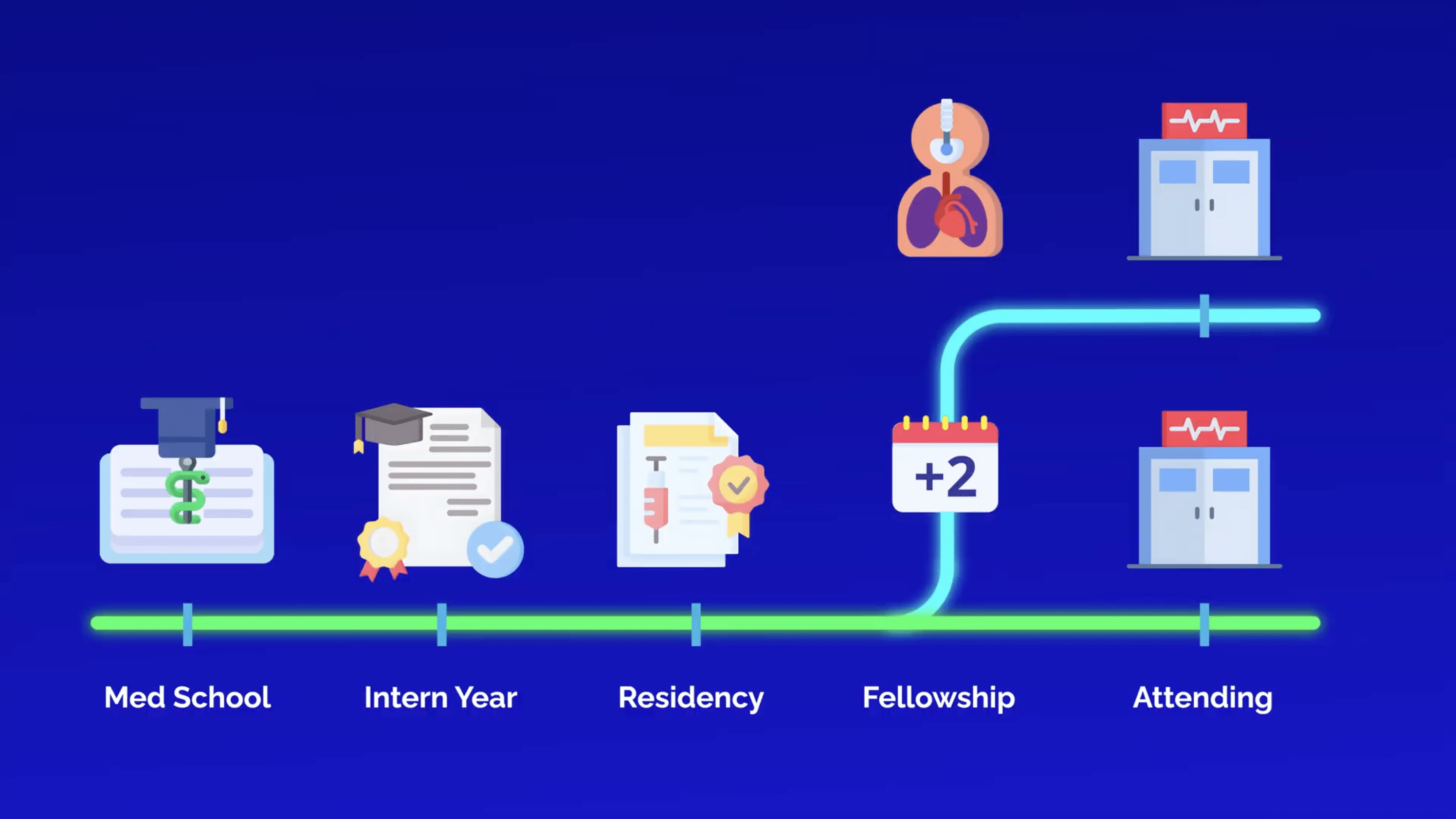
Let’s explore the fellowship options for anesthesiologists, including when additional training is required. Because after four years of medical school, an intern year, and three years of specialized anesthesia training in residency, adding yet another year or two to your education can feel daunting.
Let’s start with the benefits and drawbacks of additional training for an anesthesiologist.
General anesthesiologists are already in high demand throughout the country, so you won’t struggle to find work if you choose not to do a fellowship.
And in fact, most don’t. If you want, you can finish residency and go straight into the OR, where you’ll earn an average salary of over $490,000 and enjoy a solid work-life balance.
But for some, subspecialization opens doors to academic careers, even higher pay, niche practice settings, or simply the kind of clinical work they love most.
Consider pursuing an anesthesia fellowship if you:
But it’s not all upside. Doing a fellowship also means:
So, what are the subspecialty options for anesthesiology?

First up is adult cardiothoracic anesthesiology.
This fellowship puts you at the center of high-stakes cardiac surgeries, which often have the highest risks and rewards. You’ll master transesophageal echocardiography and become the go-to expert for unstable patients on cardiac bypass.
Transesophageal echocardiography, or TEE, is an ultrasound of the heart. But instead of placing the ultrasound probe directly on the patient’s chest, the probe is carefully navigated into the patient’s esophagus, providing a more detailed view of the heart while the surgeon is operating.
This procedure is especially important in valve replacements or bypass surgeries, and mastering TEE is a big part of the fellowship. It’s one of the key tools that make you essential in the OR for complex heart surgeries.
This fellowship is most commonly a one-year ACGME-accredited program, and it’s especially valuable if you want to work at a major academic center or national heart hospital where the sickest patients go.
The pay is higher than in general anesthesiology, but expect longer hours and more high-intensity cases.
Most anesthesia fellowship programs are ACGME-accredited, which means they’re officially recognized, standardized, and lead to board certification.
However, some anesthesia fellowships aren’t ACGME-accredited, which means that although you get the extra training and master key skills, they don’t offer board eligibility, and you might not be as readily accepted if you move to a different hospital.
If you’re looking for structured training with formal certification, ACGME is the better option, though they tend to be more competitive to match into.
Next is pain medicine, which is the most popular anesthesiology fellowship, and for good reason.
A pain medicine fellowship-trained anesthesiologist often trades the OR for the clinic. Their day involves treating patients with chronic pain by performing image-guided procedures like epidural steroid injection, nerve blocks, and spinal cord stimulators.
One of the most common procedures is a single-injection lumbar epidural steroid injection.
Under fluoroscopy, a needle is guided into the epidural space near a compressed nerve root, and steroid medication is injected to reduce inflammation and pain. These steroid injections can delay or prevent spine surgery for some patients, making them an important step for those with chronic back pain.
Pain medicine is precise, outpatient-heavy, and procedural, and the lifestyle is great. Many pain specialists work 4-day clinic weeks with minimal to no call.
As it tends to be more procedure-based than other fellowships, it’s one of the most lucrative subspecialties in medicine. Many graduates end up in private practice, with higher autonomy and income than those in OR-based anesthesiology.
The trade-off is less acute care, less OR time, and more clinic-based work. For some anesthesiologists, these are deal breakers. But if you want a lifestyle-oriented and procedure-heavy specialty with strong earning potential, pain medicine is hard to beat.
Next up is pediatric anesthesiology, which prepares you for everything from neonates in the NICU to teenagers needing routine tonsillectomy surgery.
By the way, whenever you see the suffix “-ectomy,” know that it means the surgical removal of that organ or tissue.
The physiology of pediatric patients is different. The dosing is different. And the emotional stakes are most definitely different.
Take fluid management. Children have higher metabolic rates and smaller blood volumes, so even a minor loss of fluid during surgery is dangerous. And anesthesia drug dosing becomes all weight-based, meaning tiny errors matter more. Even basic procedures, such as intubation or IV placement, become more challenging due to narrower airways and smaller blood vessels.
This fellowship is all about high precision and high empathy, creating constant demand at top children’s hospitals. That said, the pay may be slightly less than general anesthesia, as most pediatric procedures are reimbursed at a lower rate since they are assigned fewer Relative Value Units, or RVUs.
Curious about how physicians are paid? Read our guide on the RVU payment system.
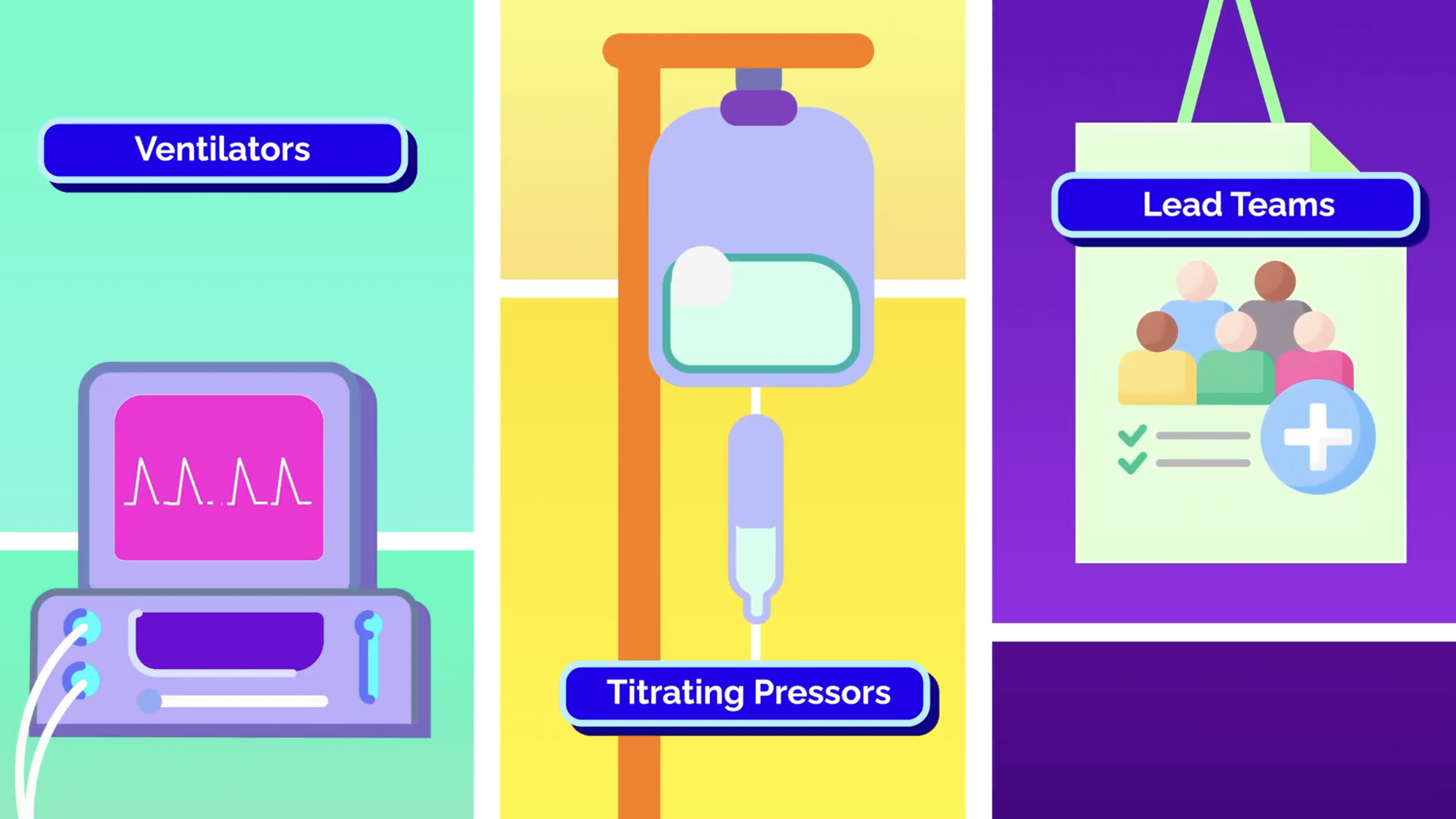
Next up is critical care medicine, which involves managing ventilators, titrating pressors, and leading multidisciplinary teams within the ICU. You’ll learn procedures like bronchoscopy, chest tube placement, and advanced line placements.
It’s a one-year fellowship, and the demand is high, especially because intensivists are always needed to help run ICUs.
Also, as an anesthesiologist, you’ll already be an expert on resuscitation and life-saving measures compared to the other specialists applying to critical care fellowship programs. This often means more fellowship interviews and better control over where you end up.
Another perk is the work-life balance. There are plenty of jobs where you are scheduled for one week in the ICU, one week in the OR, and then one week off.
This fellowship is also one of the few ways an anesthesiologist can branch back into inpatient medicine, if you’re looking for a balance between OR and inpatient.
But since not many anesthesiologists are interested in shifting back towards inpatient medicine, critical care tends to be one of the less competitive fellowships.
And then we have obstetric anesthesiology. From epidurals to emergency C-sections, OB anesthesiologists are vital physicians on the labor and delivery floor, where the pace can instantly swing from slow to chaos.
One moment, you’re placing an epidural catheter, which involves finding the correct lumbar space, carefully threading in a catheter, and delivering continuous local anesthetic to alleviate the tremendous pain of childbirth.
This high-precision catheter helps a laboring mother stay awake, pain-free, and in control, ultimately allowing them to enjoy the precious first moments with their newborn.
But minutes later, you might be rushing to the OR for an emergency C-section, where you will be expected to make decisions that impact both maternal and fetal safety.
This fellowship focuses on managing pain during childbirth, maternal comorbidities, and rare but life-threatening emergencies like amniotic fluid embolism.
It’s a niche field, and many general anesthesiologists already do OB without a fellowship. That said, fellowship makes you the go-to expert in managing complex maternal cases, and at some smaller hospitals, they will schedule their planned C-sections based on your availability.
Hospitals with high-risk obstetrics often prefer fellowship-trained anesthesiologists, and the extra training comes with a pay bump. Plus, compared to general anesthesia, you can expect more predictable hours with fewer overnight surgeries than other fellowships.
But the emotional pressure is real, as there are two lives on the table.
Next up is regional anesthesiology and acute pain medicine, which focuses on nerve blocks and catheter placements for post-operative pain control, everything from single-shot femoral blocks to continuous paravertebral catheters.
Imagine a patient who just had 5 rib fractures from a motorcycle crash. Oral meds aren’t enough, and systemic opioids are too risky for the patient’s already strained breathing.
This is where a regional anesthesiologist comes to the rescue. In this situation, they can place a continuous paravertebral catheter, a nerve catheter that’s inserted along the spine to deliver local anesthetic near the intercostal nerves. It can continuously numb that specific region of the body for days, reduce overall opioid use, and help the patient breathe easier and recover faster.
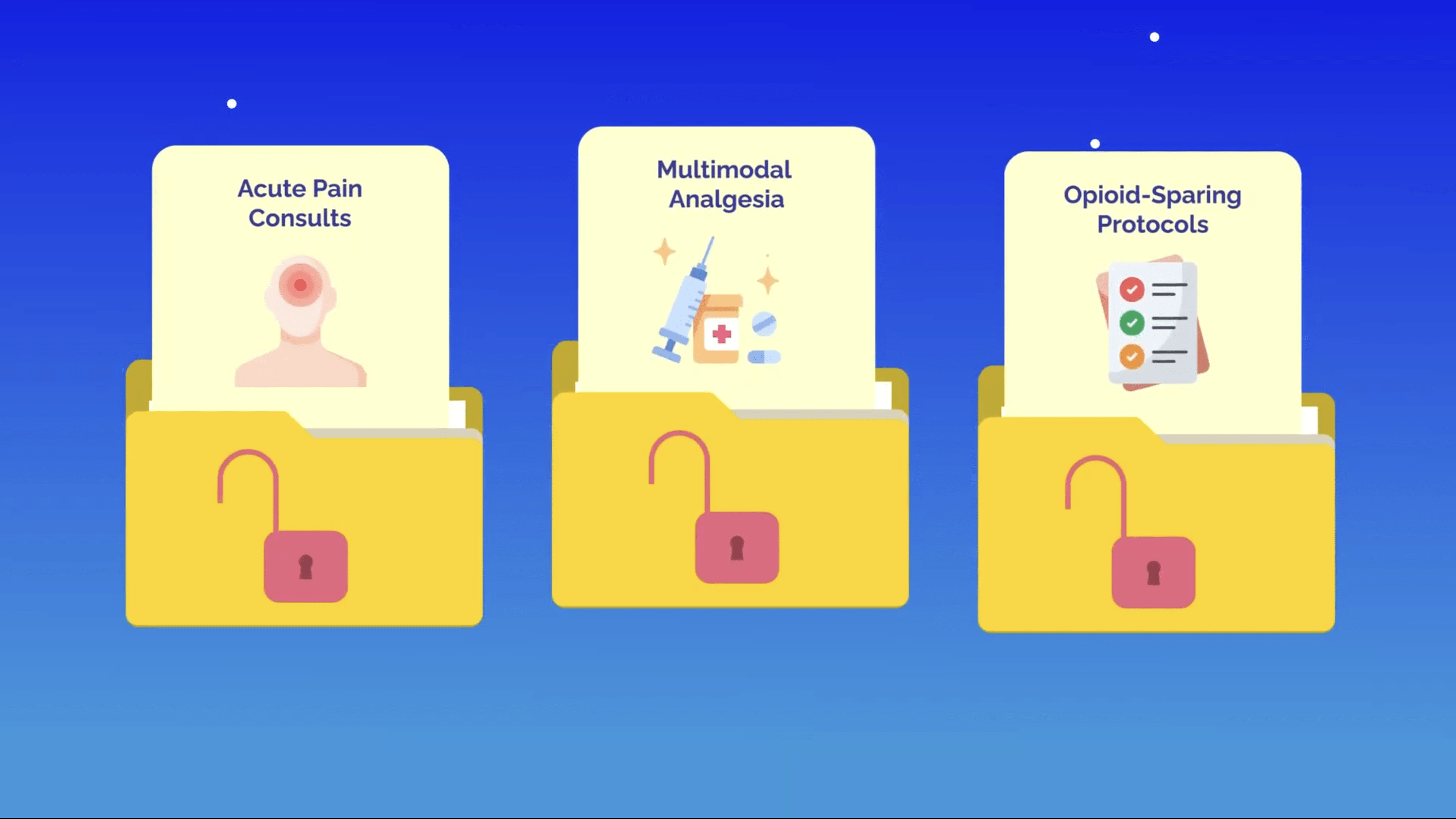
It’s an extremely hands-on fellowship, and graduates are constantly in demand at ortho-heavy hospitals and surgical centers. You’ll also gain skills in acute pain consults, multimodal analgesia, and opioid-sparing protocols.
This fellowship makes you an expert in perioperative pain management, without the grind of a chronic pain clinic.
Next up is neuroanesthesiology. While not currently an official ACGME-accredited fellowship, several established programs offer it.
Neuroanesthesiologists specialize in brain and spine surgery cases. Think craniotomies, spinal fusions, and aneurysm clippings. The most exciting surgeries are awake craniotomies.
In these surgeries, anesthesia is titrated carefully so the patient can move limbs, answer trivia questions, and even play a guitar while the surgeon removes a brain tumor.
This may sound like science fiction, but the example of someone playing a guitar during awake craniotomy surgery is absolutely real. The successful procedure was performed by neurosurgeon Dr. Sujit Prabhu. The musical performer and brain tumor survivor was Robert Alvarez.
Neuroanesthesiologists ensure that patients undergoing these procedures feel no pain. Having the patient awake and talking helps the surgeon avoid damaging vital brain regions, like speech or motor control.
It’s a delicate balance of sedation, airway management, and pain control. You’ll master neurophysiological monitoring, cerebral perfusion strategies, and tight hemodynamic control.
Fellowships are usually one year and often based at academic centers. While you can do neuro cases as a generalist, this additional training helps you build a focused niche and gets you into the bigger, more difficult neurosurgery cases.
And last but not least, transplant anesthesiology. These specialists are called in for some of the most complex, high-stakes surgeries, like liver, kidney, heart, and lung transplants.
This non-ACGME fellowship is focused on high-acuity and deeply procedural anesthesia.
A day as a transplant anesthesiologist could begin at 2 am, when a donor organ suddenly becomes available. You arrive at the OR with short notice, where you immediately begin managing massive fluid shifts, blood products, coagulopathies, and sometimes cardiac bypass.
Most transplant anesthesia programs focus primarily on liver transplants. Unlike the heart and lungs, which can be temporarily replaced by ECMO, and the kidneys, which can temporarily be replaced by dialysis, there is no replacement for the liver. These cases are notorious for being long, bloody, and physiologically complex, as you will have to manage minute-by-minute changes to vasodilation, acidosis, and coagulopathy all at once.
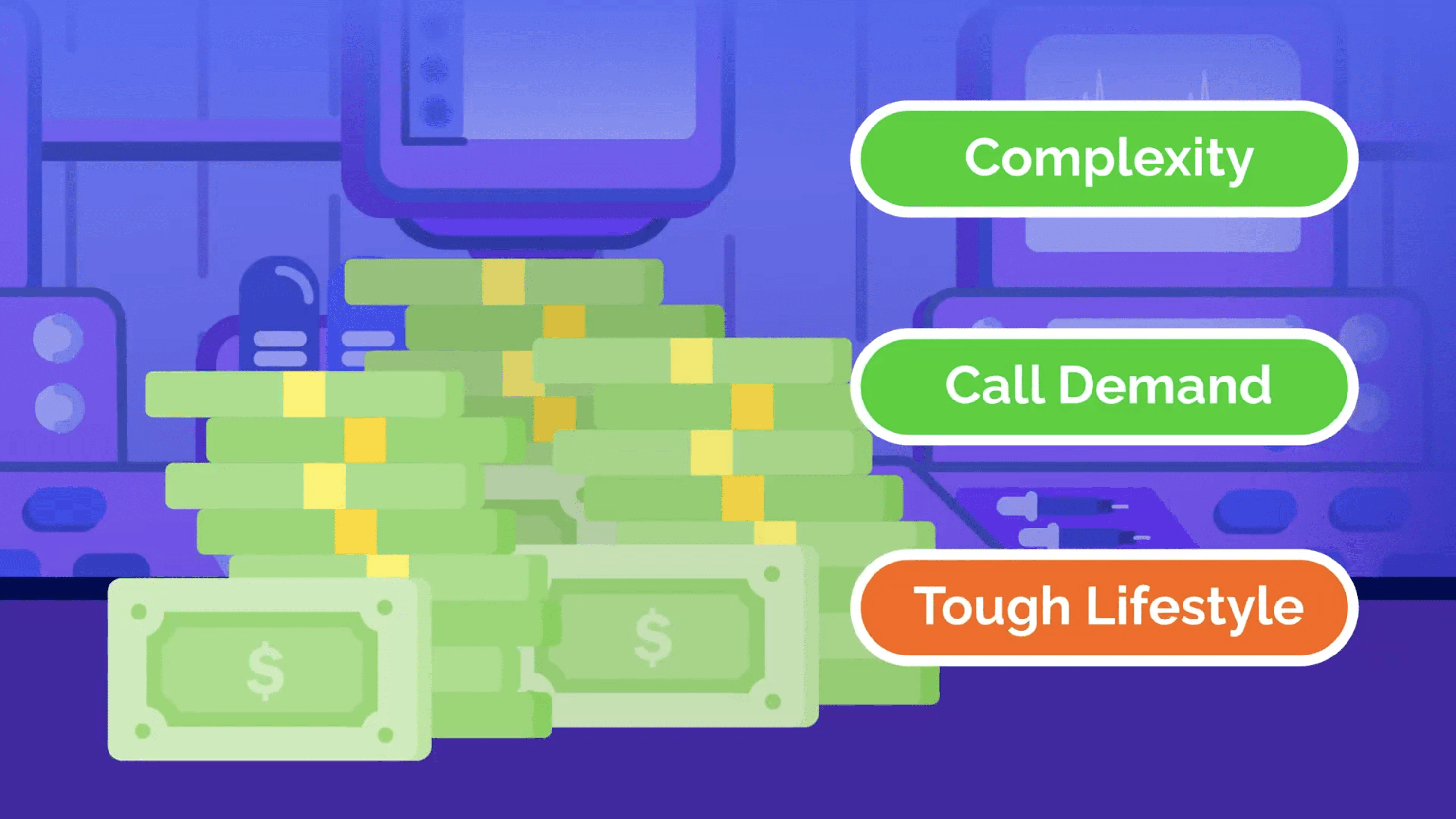
Salaries tend to be higher due to the complexity and call demands, but the lifestyle is tough. Organs don’t operate on a 9-to-5 schedule, and you’re often on call for urgent cases every couple of days.
Transplant anesthesia is not for everyone, which is made clear by the small fraction of anesthesiologists pursuing this fellowship on a yearly basis. But if you like working with some of the sickest patients in the hospital, quickly solving challenging physiology, and high-impact work, this might be your calling within anesthesia.
So, is an anesthesiology subspecialty worth it? That depends on you.
If you love variety and flexibility, general anesthesia can be an incredible, high-paying career and requires no extra training. But if you’re drawn to specific patient populations, procedures, or lifestyles, fellowship can open up a career that is more fulfilling.
But before you can set your sights on fellowship training, you’ll first need to complete a 4-year anesthesia residency, which continues to become more competitive to match into.
So, what actually makes a specialty competitive? It’s not just one thing—multiple factors come into play.
That’s exactly why we created the Residency Predictor, a free tool designed for both premed and medical students to get a more accurate read on their chances.
The tool pulls from official NRMP data and analyzes key factors like your Step 2 CK score, AOA status, number of research items, whether you attended a top 40 NIH-funded program, and even the overall match rate for your target specialty.
It doesn’t just give you raw numbers—it compares your stats against national averages and offers personalized insights on what you can improve to become more competitive.
It’s completely free, and I’m incredibly excited to finally be able to share it with you.
Check it out for yourself at ResidencyPredictor.com.

Medicine is a much wider field than most people realize. These are 12 niche doctor specialties you’ve probably never heard of.
ERAS just revamped its research section. Here’s why the arms race isn’t slowing down and what it means for your residency application strategy.



